社会学系李晓谕老师与合作者社会学系王宇航,李不群,张成岗老师,宾夕法尼亚州立大学 Orfeu M. Buxton,布莱根妇女医院和哈佛医学院Susan Redline撰写的论文《Group-based sleep trajectories in children and adolescents: A systematic review》近日发表于《Sleep Medicine Reviews》。
该研究系统回顾了利用潜在轨迹模型(latent trajectory modeling)调查0-18岁儿童和青少年睡眠轨迹的研究,并总结了相关的决定因素和健康相关结果。李晓谕老师为本文通讯作者。
原文链接:https://doi.org/10.1016/j.smrv.2024.101916
Group-based sleep trajectories in children and adolescents:
A systematic review
王宇航,清华大学社会学系
李不群,清华大学社会学系
张成岗,清华大学社会学系
Orfeu M. Buxton,宾夕法尼亚州立大学
Susan Redline,布莱根妇女医院和哈佛医学院
李晓谕(通讯作者),清华大学社会学系
Abstract
Sleep is crucial for health and development. Evidence indicates that sleep changes over time and distinct subgroups may experience different longitudinal patterns. This study systematically reviewed the studies that used latent trajectory modeling to investigate sleep trajectories of children and adolescents aged 0–18 years, and summarized the associated determinants and health-related outcomes. We searched PubMed, Embase, CENTRAL, PsycINFO, and Web of Science, identifying 46 articles that met our criteria. To ensure the reliability of the review, only studies rated as good or fair in terms of methodological quality were included, resulting in a total of 36 articles. Group-based trajectories were identified on several sleep dimensions (i.e., sleep duration, general and specific sleep problems, and bed-sharing behavior) and three or four trajectories were reported in most studies. There was a convergence trend across sleep duration trajectories during the first six years of life. Studies on specific sleep problem (i.e., insomnia, night-waking, and sleep-onset difficulties) typically identified two trajectories: consistent, minimal symptoms or chronic yet fluctuating symptoms. Lower socioeconomic status, maternal depression, and night feeding behaviors were the most frequently reported determinants of sleep trajectories. Membership in a group with certain adverse patterns (e.g., persistent short sleep duration) was associated with increased risks of multiple negative health-related conditions, such as obesity, compromised immunity, neurological problems, substance use, or internalizing/externalizing symptoms. Generally, there is potential to improve the quality of studies in this field. Causality is hard to be inferred within the current body of literature. Future studies could emphasize early life sleep, incorporate more assessment timepoints, use objective measures, and employ experimental design to better understand changes of and mechanisms behind the various sleep trajectories and guide targeted interventions for at-risk subpopulations.
缩写对照表 |
PRISMA |
Preferred reporting items for systematic reviews and meta-analyses |
PROSPERO |
International prospective register of systematic reviews |
NOS |
Newcastle-Ottawa quality assessment scale for cohort studies |
GRoLTS |
Guidelines for reporting on latent trajectory studies |
LCGA |
Latent class growth analysis |
GMM |
Growth mixture modeling |
CPTM |
Conditional probabilistic trajectory model |
LPA |
Latent profile analysis |
LCA |
Latent class analysis |
BISQ |
Brief infant sleep questionnaire |
CSHQ |
Children's sleep habits questionnaire |
SRBD |
Sleep-related breathing disorder |
CBCL |
Child behavior checklist questionnaire |
ISI |
Insomnia severity index |
SAQM |
Self-administered questionnaire for the mother |
1.Introduction
Sleep is critical in promoting health, development, and well-being, especially among young people to whom it plays a pivotal role in growth and can predict later emotional and behavioral problems [[1], [2], [3]]. Sleep undergoes changes across the developmental periods [4,5]. Therefore, instead of examining sleep at discrete timepoints, efforts to understand longitudinal sleep patterns over time may shed light on factors that influence variations in sleep and their impacts on health and development [6].
To assess longitudinal changes in sleep, some research assumes that every individual follows a single, common sleep pattern and allows for individual variability about this mean sample trend [7,8]. However, there may be distinct subgroups that follow unique sleep trajectories, representing different dynamic trends in sleep over time. An emerging method to identify relevant subgroups is group-based analysis [9], which can categorize participants into latent trajectory classes [10].
An early study empirically modeled nocturnal sleep duration trajectories and identified four developmental curves among pre-school children [11]. Since then, researchers have investigated various sleep dimensions, such as sleep duration, insomnia, sleep apnea, and sleep awakening, to describe group-based sleep trajectories in children and adolescents [[12], [13], [14], [15], [16]]. Importantly, these studies have highlighted that certain subpopulations, which might otherwise be grouped together, presented different developmental patterns. For example, among infants and toddlers with sleep-disordered breathing (as opposed to those without this condition), distinctions can be made between “early-onset”, “late-onset”, and “persistent” symptoms [17]. Besides, sleep duration trajectories such as “moderately decreasing” and “rapidly decreasing” can be differentiated from the “persistent sleeping ≥8 h/day” pattern [18]. Certain adverse sleep trajectories have been found to be related to elevated risks of subsequent health outcomes, such as mental and behavioral problems [[18], [19], [20]]. The results of these analyses add to the understanding of heterogeneous changes and development of sleep among children and adolescents. Given that the identified sleep trajectories have important health implications and that sleep is a modifiable behavior and sensitive to interventions in context and environment [21], it is crucial to have a comprehensive understanding of the current knowledge on sleep trajectories.
Much of the research that explored sleep trajectories focused on childhood and adolescence [22,23], periods marked by multiple developmental stages and the most dramatic sleep changes in life [24,25]. However, the findings of these studies have not been systematically reviewed. An overview of these studies would help inform future research, clinical practice, and interventions at the purpose of optimizing sleep and related outcomes in young individuals. Therefore, this study aims to review the literature to identify studies that have used latent trajectory modeling approaches to investigate sleep patterns in children and adolescents and have explored their associated determinants and outcomes. It should be noted that the methods themselves are not the focus of this review, which have already been described before [9].
2.Methods
This systematic review was conducted according to the Preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [26]. The research protocol was registered with the International prospective register of systematic reviews (PROSPERO; registration number: CRD42023400756).
A systematic search of the literature was conducted in the following electronic databases: PubMed, Embase, CENTRAL, PsycINFO, and Web of Science. The last search was performed on March 1, 2023. Search terms were identified in collaboration with a research librarian with expertise. The detailed search strategy is reported in Supplementary Table 1.
Studies in humans were included if they 1) had a prospective longitudinal design and had sleep assessments at multiple time points; 2) used latent trajectory modeling approaches to describe sleep trajectories; 3) examined the subgroups or classes in the sample based on the identified trajectories; 4) were limited to samples of children and adolescents (aged 0–18 years); and 5) were quantitative. Studies were excluded if they 1) did not include sleep as a primary objective of the data collection process; 2) co-modeled integrated trajectories of multiple sleep indicators or sleep with other traits, but not independent sleep trajectories; 3) were not peer-reviewed research articles; or 4) were not in English. Additionally, expert commentary and opinions, conference proceedings, or protocols were excluded.
Relevant studies were screened at multiple stages. Studies that met the criteria were evaluated using two tools: the Guidelines for reporting on latent trajectory studies (GRoLTS) [27] and the Newcastle-Ottawa quality assessment scale for cohort studies (NOS) [28]. The GRoLTS provides a standard specifically for evaluating the rationality, adequacy, and transparency of group-based trajectories. It uses a list of 21 items (including subitems) to appraise whether all essential aspects (e.g., metric of time, missing data mechanism, model comparison, and plot of final solution) are well considered and reported [27]. The NOS uses a star rating system to assess the methodological quality of cohort studies based on 8 items, grouped into three main domains (selection, comparability, and outcome). Studies can be rated as good, fair, or poor quality based on scores of the three domains [28]. Studies of poor quality as determined by the NOS were excluded, ensuring the inclusion of only moderate to high quality evidence [29]. The operational details are presented in the Supplementary file.
Data of included articles were collected using a standardized form. Narrative synthesis of findings was performed focusing on the identified sleep trajectories, as well as the associated determinants and health-related outcomes. The synthesis was grouped by sleep dimensions, such as sleep duration, sleep problems, and others, in which we highlighted similarities or differences in the findings. Studies on sleep duration trajectories were reported separately for two age groups: before school-age (≤ six years old) and after school-age. Sleep problem trajectories were reported according to the types of issues. There were cases where multiple studies, such as those by Kocevska et al. [30] and Verhoeff et al., 2018 [31], conducted analyses on identical sleep trajectories derived from the same cohorts. When reviewing the number and nature of sleep trajectories, we included only the initial study from each cohort to minimize bias. When reviewing the predictors and outcomes associated with these sleep trajectories, we included all relevant studies, including subsequent ones from the same cohorts, to capture the full spectrum of factors associated with sleep patterns in children and adolescents. Meta-analyses could not be conducted due to heterogeneity in participants, assessment points, predictors, and outcome variables.
3.Results
3.1 Study Selection
The study selection process is illustrated in Fig. 1. The database searches identified a total of 4971 initial records. After duplicates removal and title/abstract screening, 289 records were eligible for full-text screening. An additional 243 records were excluded for reasons detailed in Fig. 1. Based on quality assessment, 10 article were excluded due to their low quality, leaving 36 records for narrative synthesis.

Fig. 1. Flow diagram for study selection.
3.2 Study characteristics and quality
Table 1 provides an overview of the characteristics of the included studies. Although the inclusion criteria did not restrict year of publication, all of the studies were published from 2007 to 2023. Of these, 86% were from the past 10 years (2014–2023, n = 31) and 44% were from the last 5 years (2019–2023, n = 16). The most frequently studied sleep dimension was duration, followed by sleep problems and bed-sharing behavior. Three studies analyzed both sleep duration and sleep problems [20,32,33].

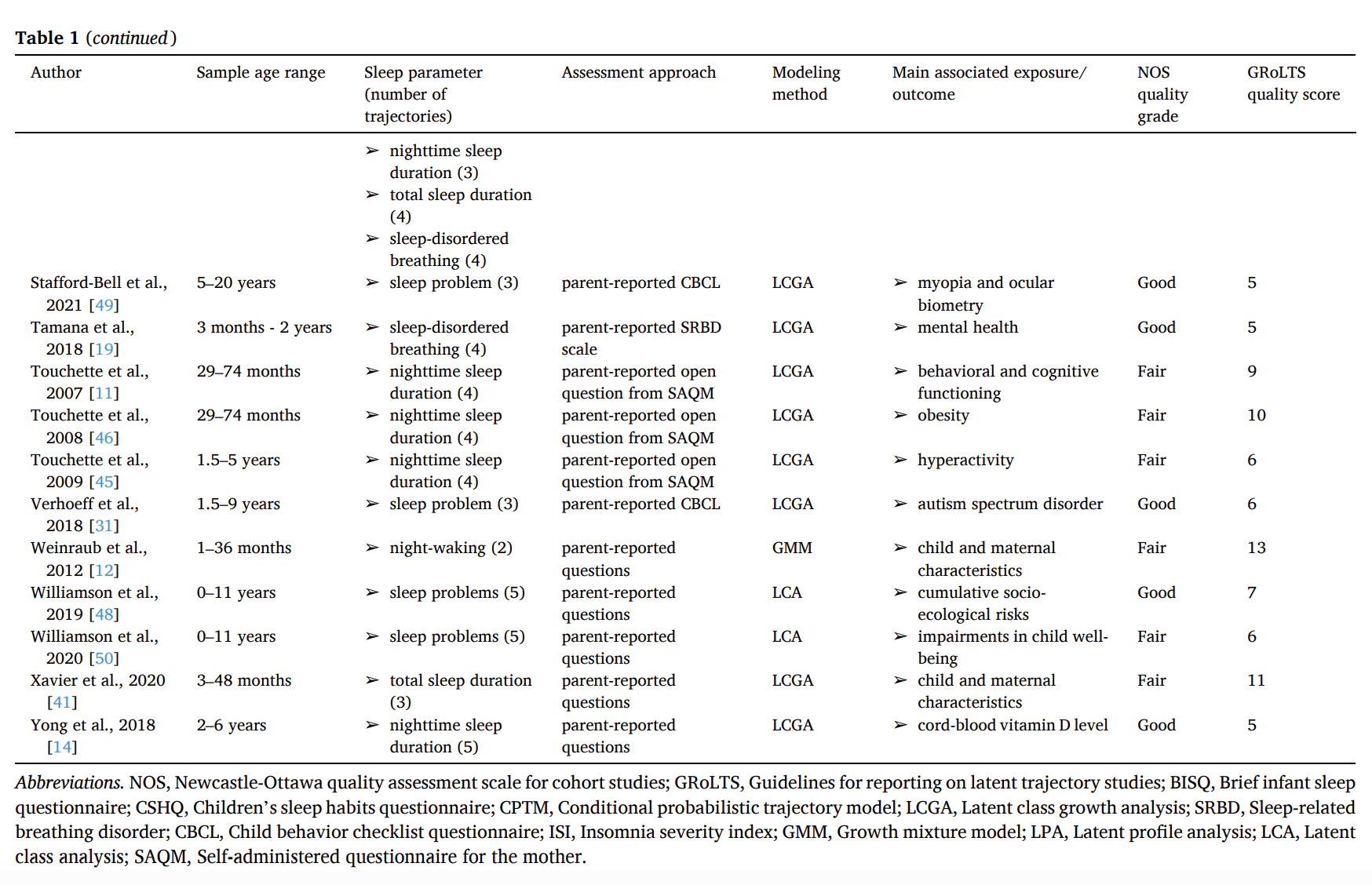
Table 1.Overview of the included articles.
Most studies were performed in upper-middle income countries (Supplementary Table 2). The study samples ranged from 243 to 7394 participants. The number of assessment points ranged from three to nine. Only one study assessed sleep objectively [34] while thirty-five studies employed parent-/self-reported sleep measurements. Latent class growth analysis (LCGA) was the most commonly used trajectory modeling method (n = 29). Bayesian Information Criterion was reported for model selection in 34 of 36 studies. Other criteria were also used, such as the average posterior probability, entropy, and group size. The sensibility, distinctiveness, and interpretability of models were also considered for model selection in several studies.
According to the NOS, 14 studies were deemed of good quality and 22 of fair quality (Supplementary Table 3). All included studies were based on prospective cohorts with relatively long follow-up durations. In 32 out of 36 studies, the retention rate of participants exceeded 60%. Only a quarter of the studies used secure assessment (objective indicators or at least validated questionnaires) for the ascertainment of both exposure and outcome. A statement of no history of incident (outcome of interest) was rarely declared at the start of the study, probably because many studies were based on birth cohorts [33,35,36]. Using the GRoLTS – a tool specifically designed for trajectory study quality assessment – none of the articles approached the perfect score of 21 with the highest score being 13 and median score being 8 (Supplementary Table 4). In all included articles, the three most commonly reported methodological details from the reporting criteria were software (item 5), covariates (item 8), and the metric of time (item 1) (Fig. 2).

Fig. 2. Percentage of studies fulfilling individual
Guidelines for reporting on
latent trajectory studies (GRoLTS) items.
3.3 Sleep duration
3.3.1. Number and nature of sleep duration trajectories
Fifteen studies modeled sleep duration trajectories, 10 of which assessed sleep in the first six years of life [4,11,20,32,[37], [38], [39], [40], [41], [42]]. Among these 10 studies, four exclusively modeled nocturnal sleep duration, two focused solely on 24-h sleep duration, and the remaining four each modeled diurnal, nocturnal, and 24-h sleep duration. All these studies relied on parent-/self-reported sleep measurements. Notably, most of these studies identified three or four trajectories. For example, one study that modeled 24-h sleep duration identified four distinct trajectories as “typical sleepers”, “initially short sleepers”, “poor sleepers”, and “persistent short sleepers” [4]. Nighttime and 24-h trajectories could show increasing, stable, and decreasing patterns. Examples of identified nighttime sleep duration trajectories were “increased”, “long persistent”, and “decreased and then increased” sleep duration [37]. Daytime sleep duration trajectories, covering age ranges from 1 to 54 months, predominantly showed a decrease with increasing age, which might be a developmentally appropriate trend [25]. Examples of identified daytime sleep duration trajectories were “decreased slowly”, “short”, and “long and decreased” sleep duration [37]. In addition, an age-related convergence of sleep duration trajectories was observed. To be specific, the variation in sleep duration across trajectories was typically larger in earlier years compared to later years. For example, one study based on participants aged from 2 to 6 years identified five nighttime sleep duration trajectories, the maximum difference between their end points was less than 1.5 h, which was half of the difference observed at the start [39]. Particularly, there were three studies evaluating trajectories in the first 24 months [20,37,42], which showed large changes for both daytime and nighttime sleep duration in early life.
Five studies tracked sleep duration trajectories beyond the commencement of school-age [18,22,34,43,44], of which four used parent-/self-reported indicators and only one measured sleep duration objectively [34]. All the five studies focused on assessing nocturnal sleep duration. Examples of identified sleep duration trajectories were “short”, “10.5-h”, and “11-h” sleep duration [22] or “persistent sleeping ≥8 h/day”, “moderately decreasing sleep”, and “rapidly decreasing sleep” [18]. Almost all sleep duration trajectories displayed a decreasing trend, regardless of their specific labels, showing that children's and adolescents' sleep duration typically reduced over time, albeit following varying slopes. In most studies, the trajectory that accounted for the largest proportion of the samples showed a slight decline in nighttime sleep duration.
3.3.2 Putative determinants associated with sleep duration trajectories
Eleven studies examined predictors of sleep duration trajectory membership [4,14,[32], [33], [34],36,38,39,41,44,45]. Among the 9 studies focusing on the first six years, two investigated the role of infant feeding status [33,36]. Jafar et al. found that formula-fed infants were more likely to be in the shorter night and total sleep duration trajectories than fully breastfed infants [36] and Murcia et al. reported that night feeding at 8 months was associated with higher risk for the trajectory of short nighttime in bed [33]. Seven other studies extensively explored potential predictors associated with membership in shorter sleep trajectories [4,14,32,38,39,41,45]. For instance, less maternal education [45], household financial difficulties [4], and maternal depression [32] were predictive to be in the shorter sleep duration trajectories. One study reported that high hyperactivity and persistently short sleep were associated; however, only joint trajectory analysis was performed and establishing causality proved challenging [45]. As for studies focusing on after school-age, one study reported that girls were less likely than boys to belong to the trajectory with shorter sleep duration [34], whereas another study based on a larger cohort found the opposite [44]. Other predictors of membership in shorter sleep trajectories included temperamental negative affectivity, low parental emotional availability, being Black or Asian, lower household income, and attending schools in large urban districts [34,44].
3.3.3. Putative outcomes associated with sleep duration trajectories
Thirteen studies researched outcomes of sleep duration trajectories [4,6,11,18,20,22,32,37,40,42,43,46,47], of which 10 focused on the first six years of life. Those with stable and/or long sleep duration trajectories were commonly used as the reference group. One study found that individuals in the persistent short sleep trajectory faced a higher risk of becoming overweight or obese compared to those sleeping for 11 h a night [46]. Five studies focused on cognitive outcomes and found shorter (especially persistent short) sleep duration trajectories detrimental to children's neurocognitive development [[11], [20],37,40,42]. Two studies reported associations between shorter sleep trajectories with externalizing problems such as hyperactivity [11,47]. Significant associations of (persistent) short sleep trajectories with immune activity [6], quality of life [4], and postpartum maternal depression [32] were also reported in individual studies. Moreover, among participants aged 6 to 18, groups with shorter sleep duration patterns had higher risks of obesity [22] and non-suicidal self-harm [18]. Another article employed dual trajectory analysis, revealing significant inter-relationships between sleep duration and cigarette smoking. The bidirectional correlation between sleep duration and cigarette smoking may exist, and the “short declining sleepers” and “escalating smokers” both showed increased levels of internalizing problems compared to other groups [43].
3.4. Sleep problems
3.4.1. Number and nature of sleep problem trajectories
Three studies analyzed trajectories of general sleep problems [15,30,48] and six studies evaluated specific sleep problems, including insomnia [16], sleep-onset difficulties [33], night awakening [12,13,32], and sleep-disordered breathing [19]. Studies tracking general sleep problems could be divided into two categories by the measurements used: parent-reported sleep problems based on a single question [48] and composite sleep problem scores based on validated scales (e.g., Child behavior checklist questionnaire) [15,30]. They examined sleep problem patterns across different developmental stages, identifying either five or three distinct trajectories. Examples of identified trajectories were “consistently minimal”, “declining”, and “persistent” sleep problems [15]. The analyses for insomnia, sleep-onset difficulties, and night awakening primarily identified two distinct trajectories: one normal trajectory characterized by consistently low levels of sleep problems, and another troubled trajectory characterized by chronic yet fluctuating sleep problems [12,13,16,32,33]. The study on sleep-disordered breathing identified four subgroups: “early-onset”, “late-onset”, “persistent”, and “no sleep-disordered breathing” [19].
3.4.2. Putative determinants associated with sleep problem trajectories
Seven studies examined determinants associated with sleep problem trajectories [12,13,17,23,33,38,48]. One study investigated predictors of general sleep problem trajectories [48]. Socioeconomic risks were linked to “mild” and “persistent” sleep problem trajectories; parental reports of distress and marital/relational hostility were associated with nearly all types of troubled sleep trajectories [48]. Meanwhile, research concentrating on specific sleep problem trajectories identified a number of putative determinants linked to the conditions. For example, passive smoking exposure, daycare in a group setting, and long-term television viewing increased the risk of being in the frequent night-waking group [12,13,23,33,38]. Predominant breastfeeding for more than 4 months was associated with belonging to the trajectory with rare sleep-onset difficulties while night feeding was linked to the membership of the “persistent common night-waking” and “persistent common sleep-onset difficulties” trajectories [33]. Kamal et al. found rhinitis and other health and behavioral characteristics associated with different sleep-disordered breathing symptom trajectories [17].
3.4.3. Putative outcomes associated with sleep problem trajectories
Ten studies investigated health-related outcomes of sleep problem trajectories [1,15,16,19,20,[30], [31], [32],49,50]. Those in the normal/rare-sleep-problem trajectory were frequently examined as the reference group. Studies on general sleep problem trajectories reported their strong correlations with adverse physical and mental health outcomes [15,30,31,49,50]. For instance, McVeigh et al. found that those in the consistently minimal problem trajectory had much lower body fat percentage and better mental health than those in the persistent problem trajectory [15]. Moreover, a study on insomnia found that the troubled sleepers had higher risks of developing internet gaming disorder and substance use [16]. Two studies found that frequent night waking trajectories were associated with maternal depression, emotional symptoms, and hyperactivity/inattention [1,32]. One study revealed that the group with persistent sleep-disordered breathing scored lower on language tests [20], and another found that early-onset sleep-disordered breathing trajectories predicted more internalizing but not externalizing problems [19].
3.5. Sleep bed-sharing behavior
One article focused on mother-child bed-sharing trajectories [35]. The study tracked participants from 3 months to 6 years old and found four bed-sharing trajectories. It reported that persistent bed-sharers had higher probabilities of showing internalizing issues, with the association stronger in those from lower socioeconomic backgrounds [35].
4.Discussion
Sleep trajectories are age-sequenced observations that reflect life-course patterns of stability and developmental change. To our knowledge, this is the first systematic review that synthesizes the literature on longitudinal sleep trajectories aimed at identifying subgroups among children and adolescents (0–18 years old), summarizing both the identified sleep patterns and their associated determinants and health-related outcomes. The recent surge in publications could be attributed to the emerging use of group-based approaches to monitor sleep patterns and the increasing availability of longitudinal sleep data. Studies have identified distinct trajectories of sleep duration, sleep problems, as well as bed-sharing behavior. Most studies have identified three or four sleep trajectories. The identified trajectories have important substantive implications.
From the studies on sleep duration trajectories during the first six years of life, a pronounced trend of convergence with age was evident [41]. To be specific, the difference between subgroups’ sleep duration patterns was larger at younger ages [42], perhaps reflecting the consolidation of sleep with development. The observation might be attributable to two factors. Firstly, there might be more initial variability in circadian rhythm development in younger children [51], which tends to become more uniform across groups with age. Secondly, as children grow, parents often adopt more structured sleep routines for them [52]. Furthermore, the introduction of daycare, kindergarten, or school routines aligns children to more uniform schedules, further narrowing sleep duration differences. With regards to the studies focusing on ages 6 to 18, nearly all trajectories depicted a decreasing trend in sleep duration as children progressed through developmental stages [22,34]. However, specific subgroups exhibited varied decreasing patterns, with the majority of individuals tracing a slight decline in sleep duration [18].
Studies for sleep problems included both general and specific types of sleep problems (e.g., insomnia [16]). Most studies that focused on general sleep problems uncovered a range of trajectories. Studies on specific sleep problems typically identified two subgroups. The majority of children and adolescents reported stable, minimal sleep issues, while a small group exhibited persistent yet variable sleep problems [13]. Importantly, the severity of the symptoms in these troubled sleepers was not anchored to static values but changed over time [12,17,32]. For instance, troubled sleepers with sleep-disordered breathing symptoms may 1) have a peak of sleep-disordered breathing symptoms in the early stages with subsequent resolution; 2) endure persistent symptoms throughout the observation span; or 3) manifest symptoms primarily in the later stages [17]. This longitudinal perspective provided a unique insight in understanding the onset and duration of sleep disorders, in contrast to the traditional static measures.
Various sociodemographic, emotional, and behavioral variables were identified as putative determinants for the shorter sleep duration trajectories and troubled sleep trajectories. Lower socioeconomic status was associated with a higher probability of being in the shorter sleep trajectories [44,45]. For example, living in a family with inadequate income (odds ratio, 2.7; 95% confidence interval [1.4,5.2]; P = 0.004) and having a mother with low education (odds ratio, 2.1; 95% confidence interval [1.1,4.1]; P = 0.03) were associated with a significant increase in the odds of being in the shorter sleep trajectories over the reference group [45]. The findings verified that longitudinal sleep patterns are not isolated but are deeply embedded within the broader socioeconomic context [44,45]. This insight might serve as a valuable addition to the Fundamental Cause Theory [53]. Emotional factors were relatively well investigated, and the results revealed that maternal depression and child high emotionality were correlated with sleep problems [13,32]. Besides, several behavioral factors, such as night feeding, passive smoking, and prolonged television viewing, were predictive of being in the troubled sleep trajectories [13,39].
Our review summarized the evidence on the associations between sleep trajectories with subsequent physical, cognitive and emotional, and behavioral outcomes. The shorter (especially persistent short) sleep duration trajectories and the troubled sleep trajectories were associated with overweight and obesity and compromised immunity [6,22]. There was a strong correlation between adverse sleep patterns with cognitive and emotional consequences, including impaired neurodevelopment, severe internalizing and externalizing symptoms, and an increased risk of developing autistic spectrum disorders [11,20,31]. One potential mechanism was that sleep problems could impede the maturational processes of the brain and neuroendocrine systems [30]. In other studies, behavioral outcomes such as substance use were also linked to suboptimal sleep patterns [16].
To ensure the scientific integrity and reliability of the evidence, certain studies were excluded from our analysis due to poor quality. Common reasons for their lower quality included the omission of important confounding variables, the lack of validated and reliable sleep measures, and the inadequate demonstration that outcome of interest was not present at baseline. The excluded studies described various sleep trajectories [54] and explored potential associations between adverse sleep patterns (e.g., high and stable sleepiness, short stable sleep duration) with a spectrum of predictors and outcomes, including body mass index [55,56], emotional/behavioral problems [[57], [58], [59]], health-related quality of life [60], parents’ relationship and family environment [61,62], and genetic factors [63]. While the observed associations add to the broader understanding of sleep trajectories, employing more rigorous methodologies is essential to establish more compelling and conclusive evidence.
Overall, sleep trajectories are arguably the premier tools, when viewed through the lens of the life course perspective [64], for assessing the dynamics of biological and behavioral evolution [65]. Sleep trajectory research has uncovered the underrecognized fact that there are meaningful subgroups within a population that follow distinctive developmental patterns [66]. Depicting an entire population with a unified average sleep trajectory oversimplifies the inherent complexities of growth patterns [10,67]. Hence, identifying and understanding group-based trajectories are among the most fundamental and empirically important research topics in medicine, behavioral sciences, and social epidemiology.
Indeed, the scientific literature on sleep trajectories and their associations with determinants and health-related outcomes has notably expanded in recent times. The value provided by latent trajectories is that it identifies various subpopulations and describes their heterogeneous longitudinal sleep patterns over time. This has at least three potential implications. First, latent trajectories are based on a rigorous methodology to ascertain sleep subgroups with smaller within-group difference and larger between-group difference. This approach reduces the reliance on subjective judgment compared to methods such as dichotomous classification and clustering analysis which might obscure complex and dynamic longitudinal patterns of sleep [68,69]. By offering a nuanced portrayal of youth sleep patterns, these trajectories facilitate the identification of high-risk subpopulations and present a comprehensive view of their developmental trends. Second, latent trajectories enhance our capacity to anticipate the temporal changes of various subgroups by equipping researchers with the tools to evaluate how risk factors or interventions might influence the evolution of these varied classes [69]. Third, trajectory as exposures may have a greater explanatory power on health-related consequences. For instance, patterns of sleep-disordered breathing were more effective to predict behavioral problems than solely considering current sleep-disordered breathing symptoms [19]. However, there are also weaknesses worthy of noting in trajectory modeling. Subjectivity can arise in choosing reference groups and interpreting subgroups’ characteristics. While most current research clearly delineated a timeline—using pre-trajectory factors for investigating determinants and post-trajectory variables for outcomes—potential bidirectional associations may still exist.
The review has strengths as the first systematic compilation on studies of sleep trajectories among children and adolescents with all types of sleep indicators, evaluated by the NOS and GRoLTS checklists. Several limitations should be noted. There is a possibility that some relevant studies were overlooked, and the review may be subject to publication bias. Due to variations in study design, sample age range, sleep parameters, length of follow up, and determinants and outcomes, the comparability of results is limited. Finally, the included studies were mainly conducted in upper-middle income countries, potentially restricting the generalizability of the findings.
Our review highlights several areas in sleep trajectory research that merit further attention. First, the majority of current studies assessed sleep only three or four times. To more accurately discern and delineate subgroups and their intricate shifts, studies should incorporate additional assessment points. Second, despite early life, especially the initial six months, being a phase of profound sleep changes in humans [24,70], it remained under-researched in sleep trajectory studies. Emphasizing newborns and infants in future research could yield critical insights. Third, present studies often focused on the link between sleep trajectories and outcomes observed at the end of these trajectories. Yet, given that childhood and adolescence are formative periods in one's development [71], the sleep patterns established early on may carry profound implications for later life. It is imperative for future research to set up long-term cohorts to explore the lasting health effects of distinct sleep trajectories among young individuals. Fourth, the literature predominantly evaluated only one or two sleep dimensions, and objective measures of sleep were underutilized, which may introduce both random and systematic biases. Future studies could study multidimensional sleep health and use tools such as polysomnography or actigraphy to objectively collect sleep data [72]. Fifth, there existed potential for improvement in both the implementation and documentation of latent trajectory analysis. For example, the appropriateness of each trajectory modeling method (e.g., GMM or LCGA) should be carefully evaluated. Each model carries its own set of assumptions and is tailored to address specific research questions. Different models applied to identical datasets can produce varying results. Sixth, bidirectional associations might exist, and causality was hard to be inferred because all included studies were observational. Experimental studies may help to provide clearer insights into the correlations observed and inform potential interventions. For example, studying the effects of a structured nightly bedtime routine within a randomized controlled trial could offer a direct examination of its impact on sleep trajectories.
5.Practice points
1.Sleep heterogeneity: Research has highlighted the diverse sleep patterns among children and adolescents, pinpointing distinct trajectories for sleep duration, sleep problems, and bed-sharing. Typically, three to four sleep trajectories were identified.
2.Sleep duration: Across studies, there was a general convergence trend of sleep duration trajectories during the first six years of life, with differences between trajectories most pronounced at younger ages and diminishing as children grew older. Most of the sleep duration trajectories during ages 6 and 18 years were declining, albeit following different longitudinal patterns at varying rates.
3.Sleep problems: Studies on specific types of sleep problems (e.g., insomnia) mostly identified two subgroups, one with consistent, low-level sleep problems and the other with chronic yet variable sleep issues. In contrast, general sleep problems exhibited a broader range of trajectories.
4.Putative determinants: The trajectories of shorter sleep duration or various sleep problems were associated with an array of sociodemographic, emotional, and behavioral determinants. The most commonly identified predictors were lower socioeconomic status, maternal depression, and night feeding behaviors. These findings may inform targeted interventions for improving sleep health.
5.Putative outcomes: Membership in suboptimal sleep trajectories, e.g., persistent short sleep duration trajectories and chronic sleep problem trajectories, was associated with subsequent adverse physical, cognitive and emotional, and behavioral outcomes. The previously underrecognized sleep trajectories might carry unique prospects in terms of identifying high-risk groups and developing interventions to improve children's and adolescents' health.
6.Research agenda
1.Assessment frequency: Future studies should incorporate more frequent assessment points to accurately pinpoint subgroups and outline the changes in their sleep patterns over time.
2.Attention to early life: More studies focusing on early life, especially the first six months of life are needed, as children experience dramatic changes in sleep during this time.
3.Long-term consequences: Future research should follow long-term health-related outcomes of distinct sleep trajectories in childhood and adolescence, which is regarded as a critical period for individuals' development.
4.High-quality measurement: More studies evaluating multidimensional sleep health and using objective sleep data are needed to enhance the overall quality and reliability of sleep trajectory research.
5.Methodological rigor: Future investigations should apply more rigorous standard when conducting and reporting trajectory modeling analysis to enhance the accuracy, interpretability, and comparability of the identified sleep trajectories.
6.Establishing causality: Studies using experimental designs are needed to better establish causality. Evidence could assist in the crafting of intervention efforts tailored to at-risk subpopulations, identified through heterogeneous sleep trajectories.




